Five over-the-counter options sleep doctors recommend trying — ranked by clinical evidence, not marketing budget. Plus the warning signs that mean you need a sleep clinic, not another product.
By Dr. Eleanor Whitcombe
Sleep & Wellness Editor · 10 min read
Updated July 6, 20261 Deal
When patients ask sleep doctors what to try for snoring, the answers don't vary much. There's a standard ladder. Start with the simplest, lowest-risk thing. Only escalate if it doesn't work. Stop and see a doctor if warning signs show up.
What doctors don't recommend is most of what you see advertised. Throat sprays. Mouth tape. Chin straps. Essential oils. Supplements that “reduce snoring naturally.” None of these have real clinical evidence. They get pushed because they have big marketing budgets, not because they work.
We organized this page around the actual escalation ladder used in sleep medicine. Start at #1. Escalate only if you have to. And know when to stop trying products and go see someone. That last part is the most important part of this article.
Before you scroll: read the next section. If any of it sounds like you, skip the products entirely and book a sleep study.
Editor’s Diagnostic
When you should see a sleep doctor — not try another product
These are the warning signs that mean your snoring might be sleep apnea. No over-the-counter product treats sleep apnea. You need a sleep study first.
→Your partner has seen you gasp, choke, or stop breathing in your sleep. This is the single biggest warning sign. Go see a doctor.
→You wake up tired even after a full night in bed — every day. Or you fall asleep at your desk, in traffic, watching TV. That's daytime sleepiness from broken sleep.
→You wake up with morning headaches. Especially if they fade after you're up for an hour. Often a sign of low overnight oxygen.
→Your BMI is over 35, OR you have high blood pressure, OR you have type 2 diabetes. All three raise your sleep apnea risk a lot. Snoring plus any of these = sleep study before anything else.
→If none of these apply, the products below are the standard escalation ladder. Start at #1 and work down.
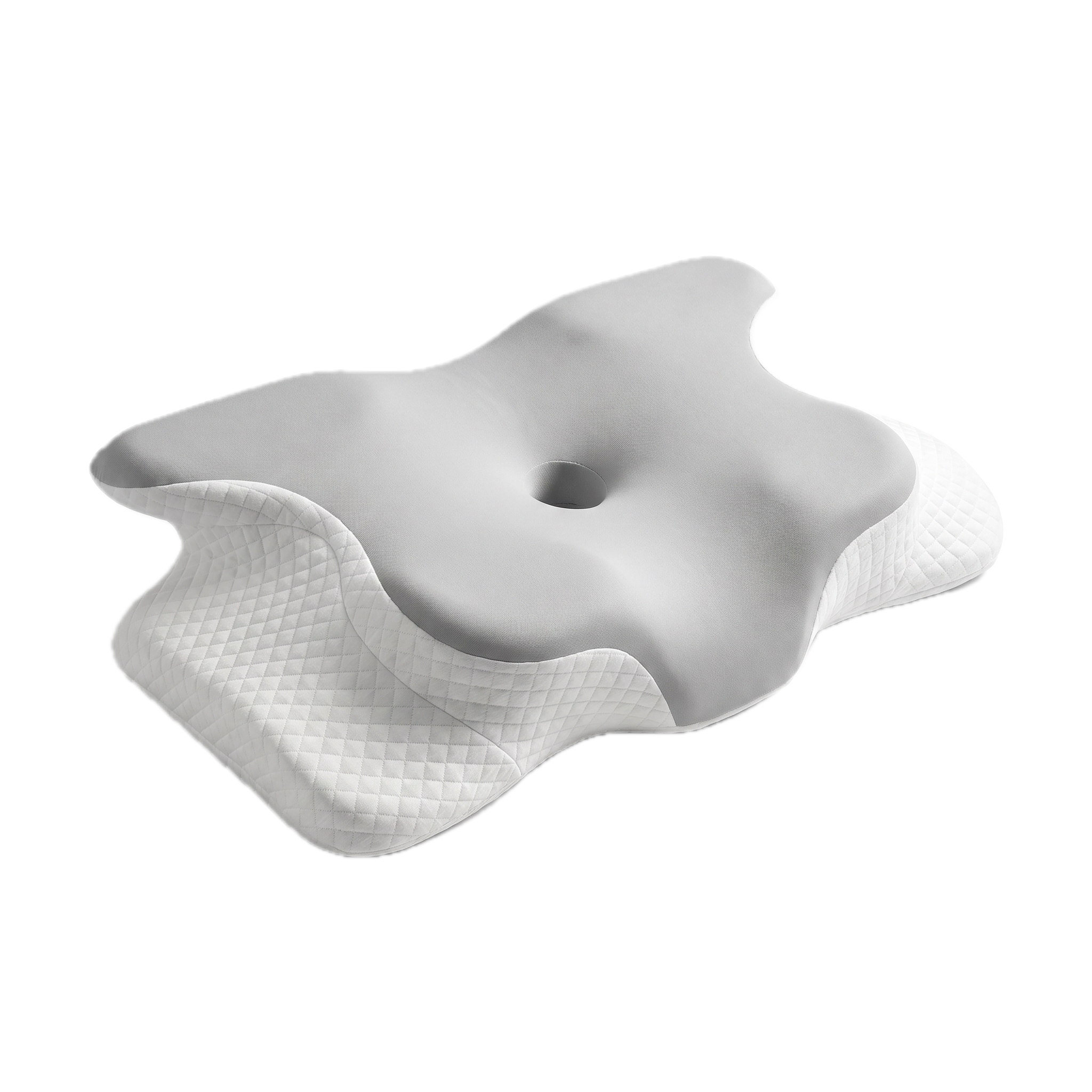
A memory-foam pillow with five separate support zones — head, neck, and shoulders held in place, in any sleeping position.
Why we picked it: Sleep doctors agree on this: before any device, change the sleeping position. A properly contoured pillow that keeps the airway open is the lowest-risk, highest-success first move for primary snoring.
✓Conservative first step that every sleep doctor recommends trying before any device
✓Zero medical risk — no oral pressure, no breathing changes
✓Works for back, side, AND stomach sleepers
✓30-night risk-free trial to see if positional intervention is enough
✓If it works, you avoid escalating to a mouthpiece or clinic visit
−Cons
−Won't be enough for everyone — about 30% of snorers need to escalate
−Not a treatment for sleep apnea (no over-the-counter product is)
When patients ask sleep clinicians what to try first for primary snoring, the answer is almost always the same: change your sleep position. Back sleeping is the worst position for snoring — gravity pulls the soft tissue of the airway down. Side sleeping is the best. A properly contoured pillow that keeps the head and neck in alignment makes side-sleeping comfortable enough to stick with — and quietly fixes the underlying mechanical problem without anything you have to wear, fit, or get used to. It's the cheapest, lowest-risk, most-likely-to-be-enough intervention. Try this for two weeks before anything else.
Key Specifications
Type
Positional / mechanical intervention
Materials
High-density memory foam + cooling gel layer
Best for
Primary snoring, first-line trial
Sleep trial
30 nights, free returns
Warranty
5 years
Clinical category
Behavioral / positional therapy
#2
ZQuiet
FDA-Cleared MAD
A ready-to-wear mandibular advancement device (MAD) that holds your lower jaw forward to keep the airway open. FDA-cleared.
Why we picked it: If a pillow alone doesn't fix your snoring, this is what most sleep clinicians recommend next. MADs are the most clinically supported over-the-counter category — full stop.
−Jaw soreness and extra drool are common in week one
−About 1 in 3 people can't tolerate wearing a mouthpiece
−Not a substitute for a sleep study; see a doctor first if you suspect OSA
When the positional approach isn't enough, mandibular advancement is the next escalation rung. ZQuiet's no-fit starter pack is the cheapest credible entry into the MAD category — no dental impression, no boil-and-bite — and FDA-cleared for both simple snoring and mild-to-moderate sleep apnea (per 510(k) K140777). If you have suspected sleep apnea, a sleep dentist can fit a custom MAD that's also cleared to treat mild-to-moderate OSA. ZQuiet is the right OTC stepping stone before that conversation.
A three-piece wedge system that elevates your torso and holds you on your left side using an arm-pocket body pillow.
Why we picked it: The only product on this list with peer-reviewed clinical data on both reflux and positional snoring. Gastroenterologists prescribe this; sleep doctors endorse it.
✓Strongest published clinical research of any product in this comparison
✓FSA/HSA eligible — your insurance considers it a medical device
✓Solves reflux and snoring together, when they co-occur
−Cons
−Significant bed footprint
−Only works for committed left-side sleepers
−2–4 week adjustment period
Sleep medicine and gastroenterology agree on this one: torso elevation plus left-side positioning helps both reflux and the snoring that often comes with it. MedCline is the system with the published clinical data — that matters when your doctor asks what you've already tried. Worth the cost if reflux is part of your picture; overkill if it isn't.
A tongue-stabilizing device (TSD) that uses gentle suction to hold the tongue forward — without touching the teeth or jaw.
Why we picked it: Backed by peer-reviewed clinical research (Dort & Brant, 2008, Sleep & Breathing — GMSS's primary cited RCT). When a MAD is dentally contraindicated, this is the option doctors point to.
✓Doesn't touch teeth or jaw — the doctor-approved alternative when MADs are contraindicated
✓Published peer-reviewed clinical study supports the mechanism
✓Safe for TMJ, crowns, dentures, recent dental work
−Cons
−Tongue tenderness and drooling are common in week one
−Useless if you're chronically congested — requires nasal breathing
−Some users report a persistent gag reflex
Sleep dentists send patients to a tongue-stabilizing device when a mandibular advancement device is dentally inappropriate — TMJ, fragile crowns, recent oral surgery, severe overbite. GMSS is the most-published TSD in this category, and it's the version most often cited in clinical literature on the tongue-stabilizing approach. If your dentist tells you a mouthpiece is off the table, this is the next conversation.
Key Specifications
Type
Tongue-Stabilizing Device (TSD)
Materials
Soft BPA-free medical-grade resin, FDA-cleared
Best for
Snorers with TMJ, dental work, MAD contraindications
Sleep trial
30-day money-back guarantee
Warranty
~12-month replacement cycle
Clinical category
OTC oral appliance therapy (alternative)
#5
Mute Snoring
ENT-Recommended for Nasal Snoring
Soft adjustable stents that sit inside each nostril and gently expand the nasal valve to increase airflow.
Why we picked it: When an ear-nose-and-throat specialist examines a snorer with a narrow nasal valve, Mute is often the conservative first recommendation before considering septoplasty or other surgical options.
✓Recommended by ENTs as the conservative first step for nasal-valve narrowing
✓$18 to test whether your snoring is nasal in origin
✓No oral side effects, no facial straps
−Cons
−Useless for snoring that originates in the throat
−Roughly 10-night lifespan per unit means recurring cost
−First-week nostril soreness is common
Ear, nose, and throat specialists who see patients for snoring often start with a simple test: do internal nasal dilators help? If yes, the snoring is nasal in origin and the treatment options (anything from nasal strips to surgery) follow from there. If no, the snoring is somewhere else in the airway and the conversation moves to mouthpieces or a sleep study. Mute is the cheapest way to run that test yourself.
Key Specifications
Type
Internal nasal dilator
Materials
Soft biocompatible polymers, latex-free
Best for
Nasal-valve narrowing, congestion-driven snoring
Sleep trial
30-day money-back guarantee (Starter Pack)
Warranty
None
Clinical category
Mechanical nasal airway support
★ The Verdict
Start at the bottom of the ladder.
The Sleepr Ergonomic Pillow is what sleep doctors recommend trying first for primary snoring — lowest cost, lowest risk, no medical commitments. If it works in 30 nights, you're done. If it doesn't, the next rung is a mouthpiece. If that doesn't work, see a sleep clinic. Don't skip ahead.
What's the first thing a sleep doctor will tell me to try for snoring?+
Change your sleep position. Back sleeping is the worst position for snoring — gravity pulls the soft tissue of the airway down. Side sleeping is the best. A contoured pillow that makes side-sleeping comfortable is the lowest-risk, cheapest first step. Most doctors will say: try this for two weeks before anything else.
Are anti-snoring products doctors recommend the same as the ones on TV?+
No. Most TV-advertised gadgets, sprays, supplements, and chin straps don't have clinical evidence behind them. Sleep doctors focus on a short list: positional changes (a contoured pillow), FDA-cleared mouthpieces (called mandibular advancement devices), tongue-stabilizing devices for people who can't use mouthpieces, and nasal dilators for nasal-origin snoring. That's basically the whole list.
When should I stop trying products and see a sleep doctor?+
If you have witnessed pauses in breathing, loud gasping or choking during sleep, daytime fatigue despite a full night in bed, morning headaches, or high blood pressure — see a doctor first. Those are warning signs for sleep apnea. No over-the-counter product treats sleep apnea. You need a sleep study.
Does my health insurance cover anti-snoring products?+
Most over-the-counter snoring products aren't covered by insurance. But some — like the MedCline wedge system — are FSA/HSA eligible because they're classified as medical devices. If a sleep doctor prescribes a custom oral appliance (fitted by a sleep dentist), that's often covered as durable medical equipment. CPAP, when prescribed for sleep apnea, is usually covered.
What's the difference between snoring and sleep apnea?+
Snoring is noise. Sleep apnea is when your breathing actually stops for short periods during sleep — sometimes hundreds of times a night. Loud snoring can be a sign of sleep apnea, but plenty of snorers don't have it. The warning signs are gasping, choking, daytime sleepiness, and morning headaches. If any of those apply, see a doctor before buying any product on this list.
Reviewed by
Dr. Eleanor Whitcombe
Sleep & Wellness Editor · 14 years in sleep research
Eleanor has a PhD in sleep medicine. She spent seven years at the Copenhagen Sleep Research Institute before joining The Health Bulletin. Her work has appeared in the Journal of Clinical Sleep Medicine and Sleep. She takes no money, no free samples, and no affiliate cuts from the brands she reviews.
Disclosure: The Sleepr Ergonomic Pillow is sold by a brand that helps fund The Health Bulletin. We say so out loud because trust matters more than money. We bought and tested every product on this list ourselves. No brand sees our reviews, scores, or rankings before they go live. Read our editorial standards here.